
West Haven, CT, June 22, 2016 (Newswire.com) - Although some learning styles (such as visual, auditory, kinesthetic) may be more familiar, Kolb's Experiential Learning Styles (Kolb & Kolb, 2005) may be more valuable in healthcare both during simulated and real experiences. Kolb's Experiential Learning Styles may help explain preceptor/preceptee mismatches, differing feedback on the same learner, and learners who are having difficulty with a certain task or specialty. Understanding your learning style will help you both as a learner and as a facilitator, as how you learn is often how you teach.
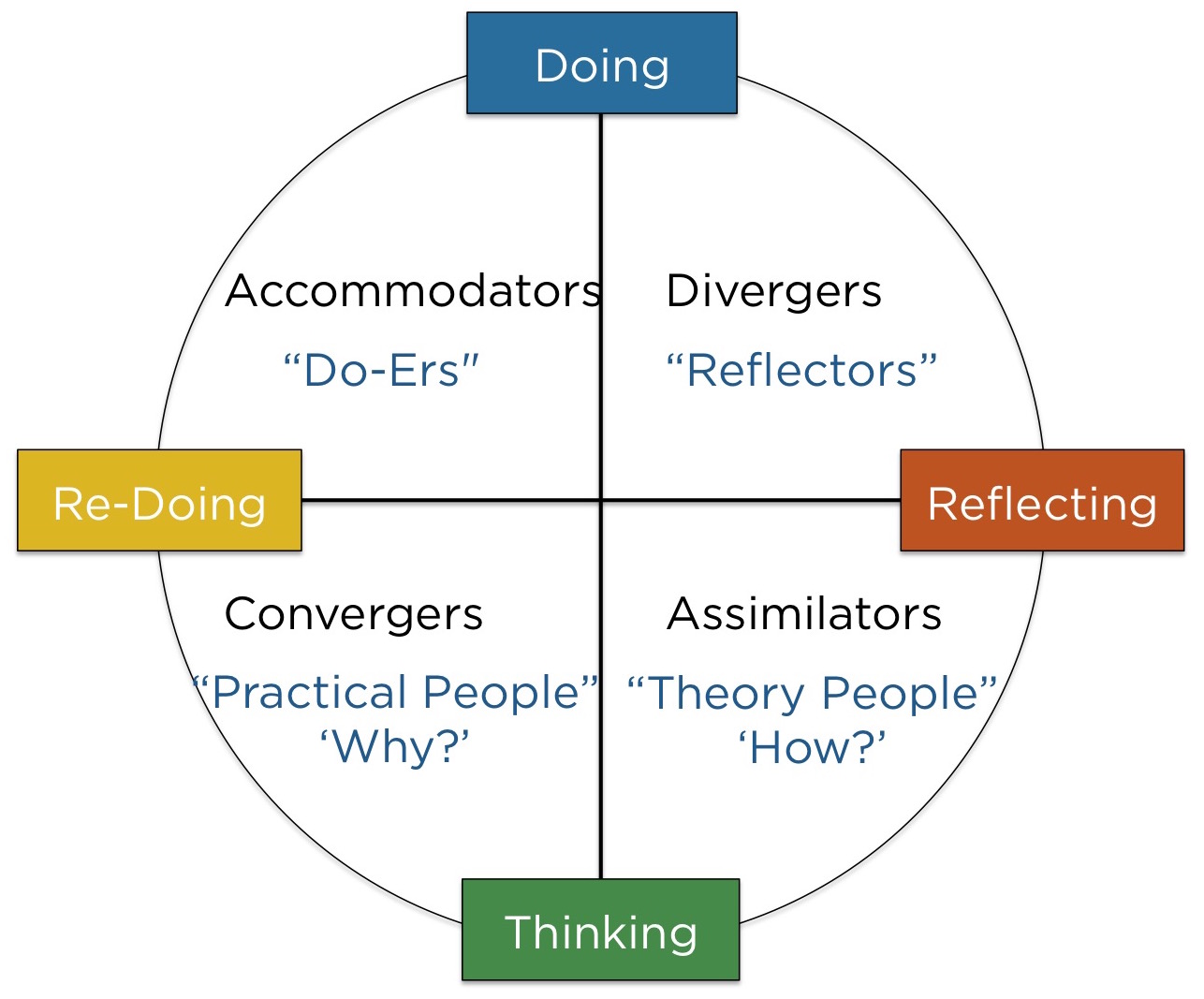
Experiential learning styles reflect the learner's preference for specific areas of the experiential learning cycle (i.e. preference for doing rather than thinking). The formal experiential learning style inventory can be purchased from the Hay Group (http://tinyurl.com/juuzqa8 ), or on Amazon at (http://tinyurl.com/h96fb8b ). The test will help you plot what your learning preferences are. If you cannot afford the test, you may find that understanding the learning styles will help you to ‘place yourself' within one or another. As with most things, Kolb has very well thought out explanations and terms for each learning style, but I prefer to ‘simplify' the styles to make them more accessible within healthcare:
Understanding your own experiential learning style in addition to the styles of your students may help to improve learning transfer and prevent conflicts in precepting.
Jay Zigmont, Learning Innovator/Founder
For about three years, I tested every resident, nurse, preceptor and anyone who took my faculty development courses using the Kolb LSI 3.1. Participants found that knowing their learning style helped them to understand their weakness (which is the opposite of their learning style), and how to approach learning in a well-rounded format. What I found interesting was that there were trends by specialty (outlined on the back of Learning Card 3a), and that learning styles may explain why facilitators rely heavily on one particular area (and why we argue so much about simulation versus lecture). Additionally, in my over 1000 responses, I found less than 10% are reflectors and learners who practice in healthcare are heavily skewed towards the practical and do-er areas.
When I see learners and facilitators with a difficulty, often it is because of their learning style (in particular when they are opposites). A facilitator who is a theorist will say that a do-er does not have ‘the font of knowledge' while a facilitator who is a do-er will say a theorist ‘just never does it.' The theorist versus do-er battle is the most obvious, as theorists tend to have a high GPA, but poor skills, while the do-er has excellent skills, but may not be able to pass the test. When learners are in areas where their faculty are all one type of learner, and they are the opposite, there is a high risk of the student failing, or dropping out, as they don't ‘fit in' (i.e. a heavy reflector may have difficulty in their surgery rotations).
As residencies move towards a competency-based model, understanding learning styles may become more important. Variation in feedback (feedforward) and scoring may be more of a reflection of differing facilitators than of the student themselves. I worked with one program where they stated that students would go to Dr. X, when they wanted to learn in the clinic, and Dr. Y when they just wanted to finish on time. Further research found that Dr. X was a reflector, and great at helping students reflect on their experience, while Dr. Y was very practical. Both physicians would give the students feedback, and would often give differing feedback regarding the same student.
Experiential learning styles may help answer the common question of "when should I lecture?" My first answer would be not to do the lecture, but if you have to, it depends on where most of your learners are. Flip classrooms (where students get the ‘lecture' outside of the classroom) are popular, but may fit reflectors best as they can complete the experience first and then get the lecture; it also may fit for theorists, who want the entire, unabridged lecture no matter what. Do-ers would rather get the experience first, and then the lecture (if they have to get a lecture at all) and the practical student wants the ‘cliff notes' of the lecture of ‘why do I care?'.
In simulation, Do-ers should be allowed to go first (and even jump in without the lecture in a safe learning environment). Reflectors would like to watch someone do it first (and tend to love debriefing). Theorists will have to be forced to do the skill (and may be experts at ‘hanging back'), while the practical learners are happiest learning something that can be immediately applied. Fortunately, good debriefing and simulation experiences will take the learner through all four areas, therefore reaching their learning style; it is just a matter of where you start.
We need to shift our advice to learners to reflect their learning styles per the below:
- Reflectors – ask your preceptor to show you once, and then you will do it.
- Theorist – ask your preceptor to explain to you how it works then you will do it.
- Practical – ask your preceptor to explain why it is important, then let you do it.
- Do-ers – ask your preceptor to let you try it first, then explain to you how or why it works.
I often provide an educational consult to learners and facilitators who are ‘having difficulty.’ The most common area related to learning styles is in test taking. As teachers, our advice for test taking is usually ‘read more,' but unfortunately that only works for theorists, and they are already reading more. The result is that we shouldn't be telling anyone to read more, and instead giving them individualized advice on how to pass a test:
- Theorists – tend not to have trouble with tests; if they do it is because they are overthinking questions (working too hard to make tacit knowledge into explicit), and may be stumped because they know too much.
- Reflectors – tend to carry ‘extra baggage' throughout a test. Because they have had previous experiences where they found an answer later in the test (i.e. the answer to number 5 at question 123), reflectors tend to mark questions to go back to them and end up in cognitive overload as they have difficulty letting questions go. Reflectors have difficulty breaking the habit, and would be better off just guessing on a question than carrying it throughout a test, as it causes errors in other questions they could know.
- Practical Learners – tend to run out of time because they are ‘fighting' the test. Practical learners often are struggling because they would ‘never do that in real life,' resulting in out thinking the test. The advice for practical learners is just to give the answer they know the test wants and stop fighting.
- Do-ers – tend to have the most difficulty on tests. Reading more does not work for them, and neither does just doing lots of questions (which is their preference). The best advice for do-ers is to have them complete a three patient review every night. Quite simply, if they take a real life patient they had in clinical and look up the diagnosis in up-to-date references they could understand the ‘why and how’ of the recent experience. It will take about an hour each night, and if they have appropriately designed clinicals, they will have reviewed the vast majority of the material before the test and not have to ‘cram' or read more.
As you dive deeper into understanding learning styles, you will be able to pick out trends without completing the assessment. You will also find that students (and facilitators) who have been struggling for years can make great improvements in short periods of time just by raising their awareness of how their experiential learning style is impacting their teaching and learning.
This part of a series called "Learning That Works" by Jay Zigmont, Ph.D., CHSE-A (jay.zigmont@gmail.com ). For a video on this topic and more information, visit http://L3a.LearningInHealthcare.com . The principles above are part of the core content (Learning Card 3a) of the Foundations of Experiential Learning Manual (http://FEL.learninginhealthcare.com ).
References
Kolb, A.Y., & Kolb, D.A. (2005). The Kolb Learning Style Inventory – Version 3.1: 2005 Technical Specifications. Haygroup: Experience Based Learning Systems Inc.
Source: Learning in Healthcare
Share: